By: Robert Shepherd MS, Certified Medical Illustrator, Vice President and Director of Eastern Region Operations, MediVisuals Incorporated
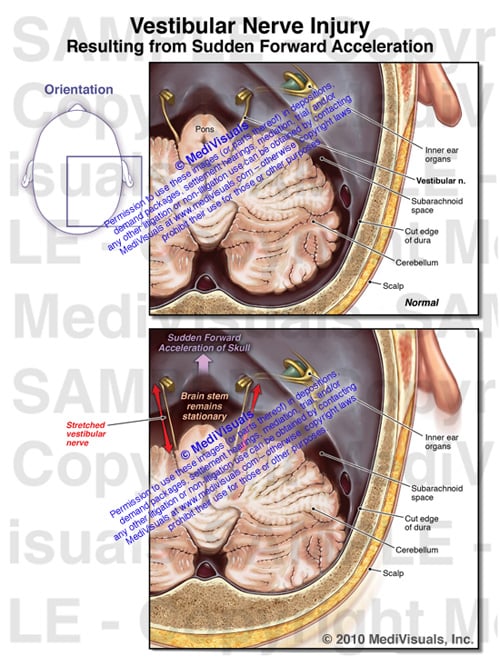
Balance and dizziness are often associated with traumatic brain injuries, although the specific cause of these problems is often difficult to explain. Sometimes the injuries may be to the inner ear organs. Other times the injuries may be to the vestibular nerve. When the injury is to the vestibular nerve, the mechanism of injury is similar to injuries to the olfactory nerve resulting in disturbances in smell.
The exhibit shown below demonstrates the mechanism of injury. As the brain stem and skull move in different directions during a violent impact, stretch injuries to the vestibular nerve can occur. This type of injury is especially significant when supporting arguments of brain injuries occurring as a result of traumatic forces to the head. If forces were significant enough to damage the vestibular nerve, the forces were likely sufficient to cause shear or traumatic axonal injury, as well.
For more information on mild and severe traumatic brain injury, please visit: http://www.medivisuals.com/traumatic-brain-injury.aspx For more information on the featured exhibit, please visit: http://www.medivisuals.com/vestibular-nerve-injury-mvi82010-01x.aspx